If you’re going to conduct surgery on the brains of children with severe epilepsy, you better know what type they have, where they have it, and how it affects function.
That’s where functional imaging comes in, including single-photon emission computerized tomography (SPECT), functional MRI (fMRI), positron emission tomography (PET), and magnetoencephalography (MEG). Most neurosurgical centers have one or two; but Children’s of Alabama has them all.
“This is important,” said pediatric neurosurgeon Jeffrey P. Blount, M.D., “because there is never perfect alignment between the studies.” With multiple studies, however, comes greater certainty about the brain regions the disease impacts, which provides greater certainty about which parts to remove during surgery. Agreement between the scans is called “concordance,” and it is the central concept in epilepsy localization, said Dr. Blount.
Most patients who require epilepsy surgery also require an invasive monitoring system prior to surgery, said neurosurgeon Curtis J. Rozzelle, M.D. In the past, he explained, that required an open cranial exposure to place electrodes on the surface of the brain and, sometimes, within the brain.
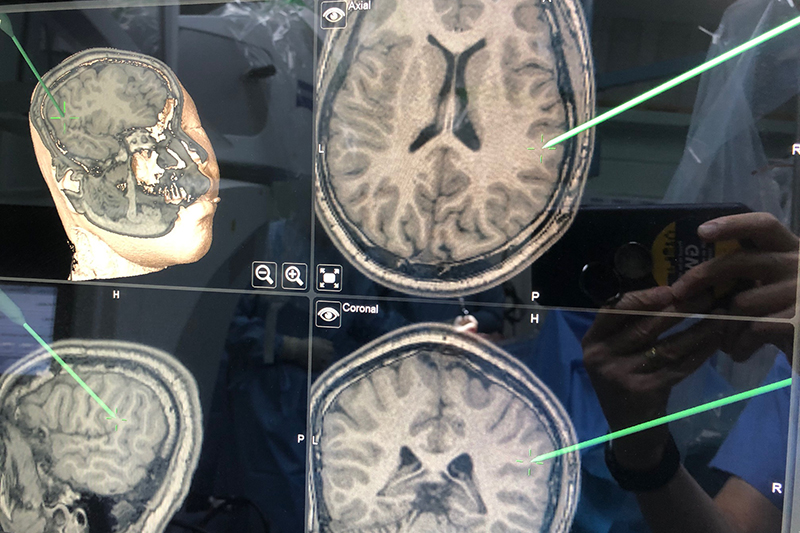
But with newer techniques, particularly stereoelectroencephalography (SEEG), a minimally invasive surgical procedure used to precisely find the areas of the brain where seizures originate, surgeons can place an array of depth electrodes without performing a craniotomy. Instead, each electrode is placed robotically through a tiny hole drilled in the skull using a robotic stereotactic approach. “That relies very heavily on high-resolution scans,” Dr. Rozelle said, including fusing CT and MRI images, to put the electrodes in without damaging a critical part of the brain.
“Mostly what we’re trying to avoid is hitting blood vessels with the depth electrodes while getting an array of electrodes that will cover the area of interest,” Dr. Rozelle said. The functional imaging studies are critical in establishing the target zones. Plus, since MEG and fMRI are based on magnetic field fluctuations, the MEG images can be mapped onto the MRI scan in three dimensions. The older technique, in which electrodes were placed on the surface of the brain, only provided a two-dimensional image.
The child spends several days with the implanted electrodes to capture data about the seizures, which a neurologist then analyzes to identify the exact area of the brain that requires treatment. That surgery itself also relies heavily on high-resolution imaging. A laser ablation, for instance, is performed in the MRI scanner. A larger-volume surgery that requires open resection also relies on imaging because the surgical target looks the same as the normal brain. “To help us ensure that we hit the target, we can map the neurologist analysis into a navigation system that directs us to the right area,” Dr. Rozzelle said. “That ensures that we remove the tissue we need to take out and keep everything else intact.”
Neurosurgeons at Children’s perform about 50 cranial epilepsy procedures a year, of which about 30 require the invasive monitoring.
“We are very fortunate to work in a center where we have so much high-quality functional imaging available on a single campus,” said Dr. Blount.